MedPAC Moves Away From Inflation-Based Physician Payments
Over the years, physician groups have been calling on Medicare to increase the rate of reimbursement, claiming that the annual payment adjustments under the program have not kept up with the actual cost of operating a medical practice.
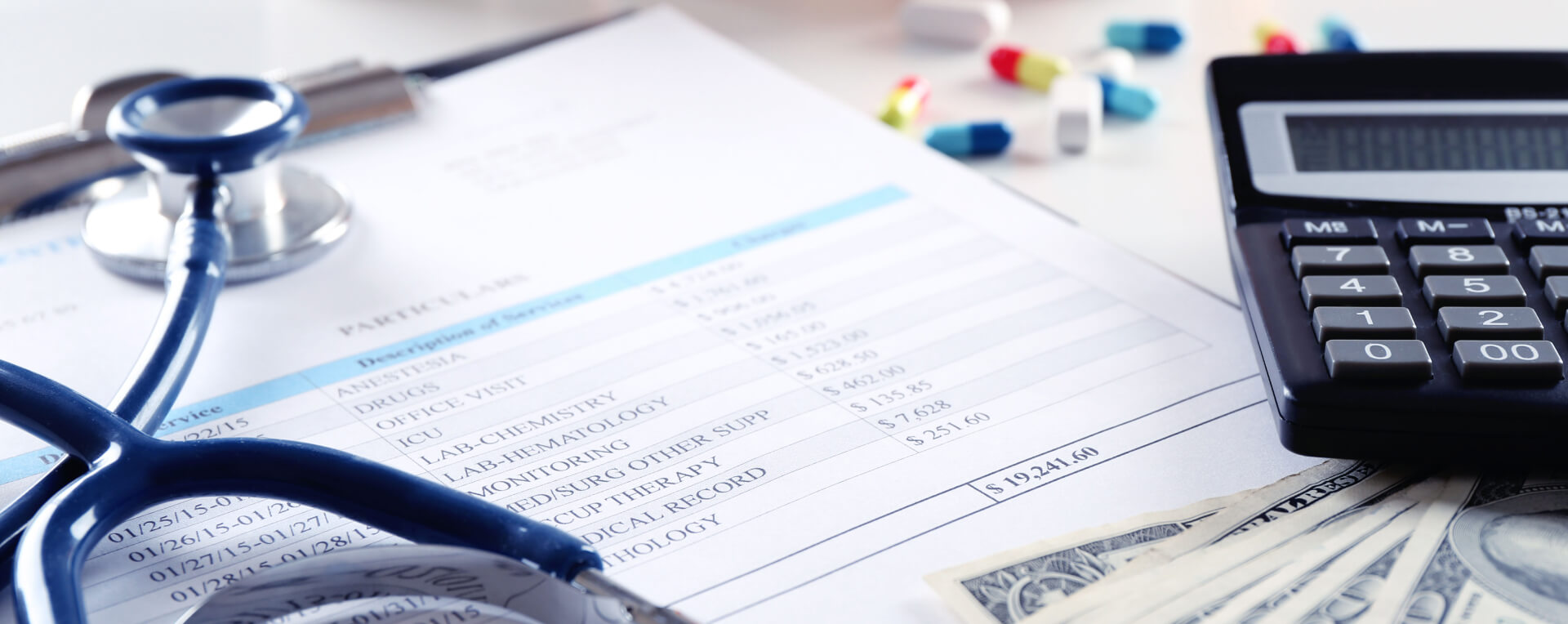
The American Medical Association reports that the Medicare reimbursement to physician practices has decreased by approximately 33 percent since 2001, when inflation is factored in. At the same time, practice expenses have continued to climb. The Medicare Economic Index (MEI), which tracks healthcare-related inflation, increased by 3.5% in 2025, adding more pressure to already tight margins.
A major reason this mismatch continues is that CMS is legally required to keep annual physician payment updates budget-neutral. In simple terms, Medicare cannot freely raise physician rates year after year without offsetting those increases somewhere else, which makes it difficult to keep up with inflation.
In many years, Congress ends up stepping in with temporary fixes. But doctors argue this pattern creates constant uncertainty. When payment changes require last-minute legislative action, practices find it difficult to plan, staff, and invest in personnel, technology, and long-term upgrades.
To add additional stability to the Medicare physician payment, the Medicare Payment Advisory Commission (MedPAC) suggested last year that Congress should tie annual payment increases to the MEI. MedPAC specifically suggested an updated formula of MEI minus one percentage point.
This proposal was intended as a middle ground. Physician groups generally supported the idea of modernizing Medicare’s payment structure, but many wanted a more generous increase, such as MEI plus one percentage point, rather than a reduction from the index.
Now, however, MedPAC appears to be moving away from that framework, which became a key reason two commissioners voted against the group’s draft recommendation for 2027.
Commissioner Kenny Kan, a New Jersey Blues health plan executive, said MedPAC’s earlier MEI-minus-one idea followed years of effort to balance two competing realities: physicians often lose money treating Medicare patients, while Medicare must also limit long-term spending growth. Kan warned that the newly proposed approach effectively results in a 2.2% payment cut for doctors.
The second dissenting commissioner, Brian Miller, an associate professor of medicine at Johns Hopkins University, also criticized the direction of the recommendation. He said the update is especially difficult to justify when Medicare tends to provide stronger payment protection for hospitals.
Miller emphasized that the proposed MedPAC guidance would result in a negative update for physicians overall, and he argued that the policy debate is missing the bigger picture.
MedPAC Chair Michael Chernew defended the draft recommendation, explaining that MEI minus one was never meant to be a strict rule. Instead, he said it was intended as a baseline reference point, with the final payment recommendation adjusted around that benchmark.
Chernew also noted that physician revenue could end up higher than what the base rate update suggests, largely due to increased billing intensity and coding-related factors that can influence total Medicare payments.
In his view, the final impact for doctors could still be slightly above the current law once those other factors are considered.
The American Medical Association reacted by accepting the update proposed by MedPAC, but questioned the commission abandoning its previous solution. AMA Board Chairman Dr. David Aizuss said in a statement that the organization was disappointed that MedPAC had reversed the position it had taken months before regarding the payment structure it endorsed.
Aizuss emphasized that linking physician updates to the MEI would allow medical practices to have long-term predictability and safeguard patient access, which is already a significant concern in rural and underserved communities with physician shortages.
MedPAC also recommended that hospital reimbursement not be reduced under current law in 2027, along with physician payment recommendations. Commissioners re-endorsed a proposed tool known as the Medicare Safety-Net Index that is meant to allocate more resources to hospitals that serve low-income and high-need patients.
Meanwhile, MedPAC voted to suggest other Medicare spending cuts. The commission supported a 4% cut to skilled nursing facilities and a 7% cut to home health agencies and inpatient rehabilitation facilities in 2027, compared to the current law.