Medicare DMEPOS Moratorium Expands as Florida Takes Additional Action
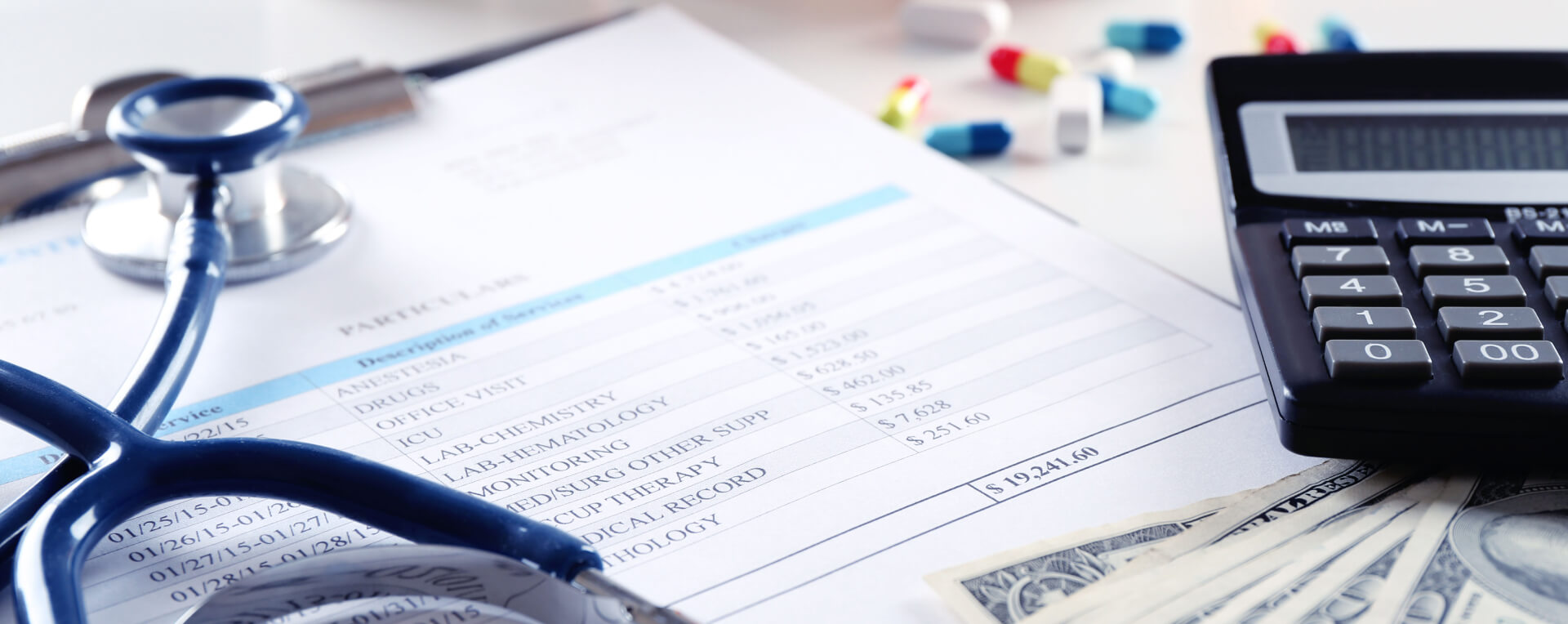
In a significant escalation of federal healthcare fraud enforcement, the Centers for Medicare & Medicaid Services (CMS) has announced a six-month nationwide enrollment moratorium on select durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) suppliers. The moratorium, effective February 27, 2026, marks the first time CMS has implemented such a restriction on a national scale.
The move aligns with a broader anti-fraud initiative under the administration of Donald Trump, following a March 16 executive order establishing the Task Force to Eliminate Fraud. The task force, chaired by JD Vance, is expected to deliver a coordinated national strategy within 90 days. CMS Administrator Mehmet Oz emphasized that the moratorium is designed to curb fraud, safeguard beneficiaries, and ensure quality care delivery.
Scope and Duration
The moratorium, currently set to run through August 27, 2026, applies to seven categories of DMEPOS suppliers classified as “medical supply companies,” including those employing orthotics, prosthetics, pedorthic personnel, pharmacists, and respiratory therapists. Initial enrollment applications submitted during this period will be denied, while those filed before the effective date remain under review.
CMS retains the authority to extend the moratorium in six-month increments under federal regulation (42 C.F.R. § 424.570), citing concerns over fraud, waste, and abuse. The agency has also warned that attempts to bypass the restrictions could result in severe penalties, including up to a 10-year re-enrollment ban and referral to oversight bodies such as the Office of Inspector General (OIG).
Expanded 36-Month Rule Complicates Transactions
Adding further complexity, CMS expanded the “36-month rule” (42 C.F.R. § 424.551) to include DMEPOS suppliers effective January 1, 2026. Under this rule, a change in majority ownership (CIMO) within 36 months of enrollment triggers a requirement for re-enrollment—effectively subjecting such transactions to the moratorium.
This development has major implications for mergers and acquisitions (M&A). Asset purchases, which typically require new enrollment, are effectively blocked during the moratorium unless buyers can delay closing or operate without Medicare or Medicaid revenue. Even stock transactions may carry risks, including exposure to historical liabilities.
Florida Implements Parallel Medicaid Moratorium
In a rapid response to CMS’s call for state-level action, Florida became the first state to implement a Medicaid-specific DMEPOS enrollment moratorium. Approved by CMS and announced on March 25, 2026, the state’s freeze took effect retroactively from March 20 and will remain in place through approximately September 20, 2026.
Issued by the Florida Agency for Health Care Administration (AHCA), the moratorium applies broadly to DME providers (provider type 90) across all counties. Similar to the federal rule, it excludes pharmacies, hospitals, and providers for whom DME services are not a primary function.
Applications submitted before March 20 will continue to be processed, while existing providers may maintain operations and billing. However, the delayed issuance of AHCA’s alert five days after the effective date has raised concerns that some providers may have unknowingly submitted applications during the restricted period.
Misalignment Between Federal and State Policies
The federal and Florida moratoria are not fully synchronized. While the CMS restriction ends on August 27, Florida’s extends nearly three weeks longer, potentially creating operational uncertainty for suppliers operating in both programs.
Additionally, CMS’s moratorium targets specific supplier categories, whereas Florida’s applies broadly without subcategory distinctions. This divergence may result in suppliers being restricted under one program but not the other.
Market and Managed Care Implications
The dual moratoria significantly restrict market entry in Florida, particularly affecting suppliers serving dual-eligible populations. With most Medicaid beneficiaries enrolled in managed care, the inability to onboard new suppliers could strain network adequacy and shift negotiating leverage toward existing providers.
Managed care organizations (MCOs), which require Medicaid enrollment prior to credentialing, may face challenges in maintaining sufficient provider networks during the moratorium period.
| Element | Florida Medicaid Moratorium |
| Effective Date | March 20, 2026 |
| Duration | Initial six-month period (through approximately September 20, 2026) |
| Scope | DME providers (provider type 90) in all Florida counties |
| Exclusions | Pharmacies, hospitals, or other medical providers that provide DME as a “secondary function.” |
| Pending Applications | Applications submitted on or before March 20, 2026, will continue to be processed |
| Existing Providers | May continue to deliver and bill for authorized services |
Enforcement and Compliance Expectations
CMS has signaled intensified oversight across all program integrity areas, including enrollment verification, billing practices, site inspections, and ownership disclosures. The agency continues to exercise strict enforcement of DMEPOS supplier standards, with even minor compliance failures potentially leading to revocation and re-enrollment bars.
Suppliers are advised to maintain rigorous documentation, conduct internal audits, and prepare for heightened scrutiny. Engagement with legal counsel is recommended in the event of inquiries from CMS, the OIG, the Department of Justice, or state Medicaid Fraud Control Units.
Outlook
CMS’s invitation for states to adopt similar Medicaid moratoria suggests that additional states may follow Florida’s lead. Jurisdictions with historically high levels of DME fraud—such as Texas, California, and Michigan are considered likely candidates.
As regulatory activity accelerates, DMEPOS suppliers, investors, and healthcare stakeholders must closely monitor federal and state developments and reassess compliance strategies, transaction structures, and market entry plans in a rapidly evolving enforcement environment.